Mortality and morbidity linked to smoking
- It is estimated that in Switzerland, nearly 9,500 people died from smoking-related diseases in 2017, which represents more than 26 deaths each day over the course of the year.
- The mortality rate attributable to smoking was 112 deaths per 100,000 inhabitants in 2017. Smoking was thus the cause of 14.2% of all deaths in Switzerland that year.
- In 2017, 29% of the deaths attributable to smoking were linked to lung cancer, 16% to other types of cancer, 17% to Chronic Obstructive Pulmonary Disease, 17% to heart disease, and 9% from other smoking-related diseases.
- Premature death linked to smoking also affect relatively young age groups. In 2015, no fewer than 480 individuals ages 35 to 54 years old, and 1,258 people ages 55 to 64, died prematurely from smoking-related illness.
- In addition to deaths, certain curable diseases can be attributed to smoking, whether totally (smoking being the only cause; 100% responsible), mostly (partly due to smoking, estimated between 75% and 99% responsible), or partially (estimated at less than 75% responsible).
- With more than four hospitalisations annually for 1,000 inhabitants, mental and behavioural problems related to tobacco use are the most common diagnoses totally attributable to tobacco use.
- Among the diagnoses which are principally due to tobacco use (between 75 and 99%), the most common are tachycardia, atrial fibrillation and atrial flutter, and other heart arrhythmias (> 7 hospitalisations annually/1,000 inhabitants) and bronchitis, emphysema, and other chronic obstructive pulmonary diseases (>4/1,000 inhabitants) are the most frequent.
- Almost a quarter – 23.4% – of daily smokers report dealing with moderate to serious psychological problems.
Globally, it is estimated that in 2019, smoking caused 7.7 million deaths (GBD 2019 Tobacco Collaborators, 2021[1]). In fact, smoking is one of the biggest risk factors for death and for non-communicable diseases (NCDs). For example, smokers in Switzerland presented not only a greater risk of death from cancer than non-smokers, but also from cardiovascular and other diseases (non-cancerous and non-cardiovascular) (Maag et al. 2013[2]). Also, around a quarter of people who begin smoking young and continue into adulthood will die from a smoking-related illness between the age of 35 and 69, and another quarter will die early from these illnesses after the age of 70 (Doll et al., 2004[3]). On average, according to these models, smokers lose 10 years of their lives compared to non-smokers.
Mortality: 9,500 deaths per year in Switzerland
The latest estimates of the mortality rate linked to tobacco use in Switzerland are for the year 2017 (OBSAN, 2022[4]). It is estimated that 9,496 premature deaths that occurred that year were due to smoking, which corresponds to 14.2% of the total number of deaths for that year. Thus, on average, more than 26 deaths a day can be attributed to smoking. The corresponding raw mortality rate is 112 deaths annually for 100,000 inhabitants. These deaths include more men than women (5,987 men versus 3,509 women), but the ratio of men to women has tended toward equality over the past few decades.
Regarding the specific causes of death due to smoking that occurred in 2017, 29% were related to lung cancer and 16% to other types of cancer (Figure B1). Chronic obstructive pulmonary disease (COPD) caused 17% of these deaths, ischemic heart disease another 17%, and other heart diseases 9%. Stroke (4% of deaths), other vascular diseases (4%), and other diseases such as pneumonia, flu, and tuberculosis (3%) and diabetes (1%) were the other causes of death related to smoking.
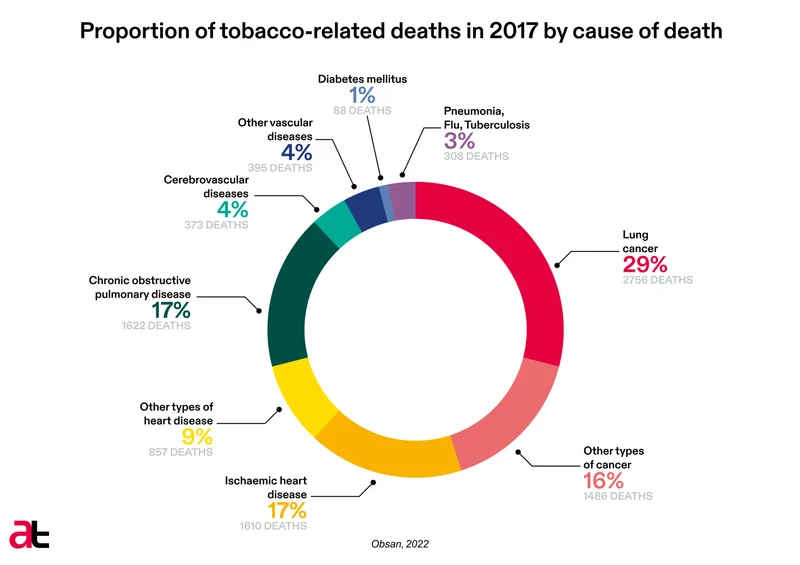
Figure B1 – Proportion of deaths attributable to smoking in 2017, according to cause of death (Source OBSAN, 2022[5]).
Detailed estimates from 2015 – the year for which there were 9,535 reported deaths caused by smoking – break down smoking-related deaths by age group (Mattli et al., 2019[6]). Although, not surprisingly, older people (ages 65 – 74 and 75 and up) were the most affected by premature death linked to smoking, no fewer than 480 people ages 35 – 54 and 1,258 people ages 55 – 64 also died prematurely from smoking-related diseases that year.
Morbidity linked to smoking
The theme of smoking-related morbidity is addressed indirectly, for example, by means of the indicator, “Consumption of substances and psychological problems” in the monitoring system for addiction and NCDs (MonAM) of the Federal Office of Public Health (FOPH) (OBSAN, 2022[7]). Based on data from the Swiss Health Survey (ESS) study from 2017, this indicator underlines the fact that, with a level of diagnosed moderate to severe psychological problems of 23.4%, daily smokers (28.6% of women and 19.2% of men) present a significantly higher propensity for these kinds of problems than people who do not use substances at a risky level[8], for whom the proportion was 13.0% (men and women combined).
Older analyses of the Statistique médicale des hôpitaux of the FOPH, looking at diagnoses from International statistical classification of diseases and related health problems (CIM) of the WHO (WHO, 2008[9]) complement the picture with information about certain morbidity factors attributable to the use of tobacco. Analysed for the Addiction Monitoring Switzerland, the data for 2008 from the Statistique médicale des hôpitaux identify mental and behavioural problems linked to tobacco use (code CIM-10 F17) as being the most common diagnoses of illnesses totally attributable to tobacco use, with more than 4.08 hospitalisations annually for 1,000 inhabitants (https://www.suchtmonitoring.ch, 2013-2022[10]). Other diagnoses completely attributable to tobacco use (toxic effects of tobacco and nicotine - and fetuses and newborns affected by mothers’ smoking; codes CIM-10 T65.2 and P04.2) were much rarer. Among the illnesses principally attributable to smoking (illness for which it is estimated the smoking is responsible for 75 – 99% of the risk), cases tachycardia, atrial fibrillation, and atrial flutter and other heart arrhythmias) (J47-J49) were the most common, with a rate of 7.22 per 1,000 inhabitants (https://www.suchtmonitoring.ch, 2013-2022[11]). They outnumbered diagnoses of bronchitis, emphysema, and other lung diseases per 1,000, and those of Cardiopulmonary and Pulmonary Circulation Diseases (I26-I28), which had 1.83 cases per 1,000 chronic obstructive – bronchitis, emphysema, and other COPDs – (J40-J44) with 4.31 cases per 1,000.
[1] GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. 2021 397: 2337-2360.
[2] Maag, Judith; Braun, Julia; Bopp, Matthias; Faeh, David. Swiss National Cohort, Direct Estimation of Death Attributable to Smoking in Switzerland Based on Record Linkage of Routine and Observational Data. Nicotine & Tobacco Research. 2013 15: 1588–1597.
[3] Doll, Richard; Peto, Richard; Boreham, Jillian; Sutherland, Isabelle. Mortality in relation to smoking: 50 years observations on male British doctors. BMJ. 2004 328: 1519-1528.
[4] https://ind.obsan.admin.ch/en/indicator/monam/tobacco-attributable-mortality; accessed 11.03.2022.
[5] https://ind.obsan.admin.ch/en/indicator/monam/tobacco-attributable-mortality; accessed 11.03.2022.
[6] Mattli, Renatoi; Farcher, Renato; Dettling, Marcel; Syleouni, Maria-Eleni; Wieser, Simon. (2019). Die Krankheitslast des Tabakkonsums in der Schweiz: Schätzung für 2015 und Prognose bis 2050. Winterthur: Winterthurer Institut für Gesundheitsökonomie, School of Management and Law, ZHAW und Institut für Datenanalyse und Prozessdesign, School of Engineering, ZHAW.
[7] https://ind.obsan.admin.ch/fr/indicator/monam/consommation-de-substances-et-problemes-psychiques-age-15-a-74; accessed 11.03.2022.
[8] More specifically: people who did not smoke daily, did not drink at a high-risk level, did not use cannabis daily or almost daily, and who had not used other illegal substances in the preceding 12 months.
[9] https://icd.who.int/browse10/2008/fr ; accessed 11.03.2022.
[10] https://www.suchtmonitoring.ch/fr/1/6-2.html?tabac-morbidite-et-blessures-maladies-totalement-attribuables; accessed 11.03.2022.
[11] https://www.suchtmonitoring.ch/fr/1/6-3.html?tabac-morbidite-et-blessures-maladies-partiellement-attribuables; accessed 11.03.2022.
AT Switzerland, September 2022